Did the Polyvagal Theory get it all wrong?!
Mar 03, 2026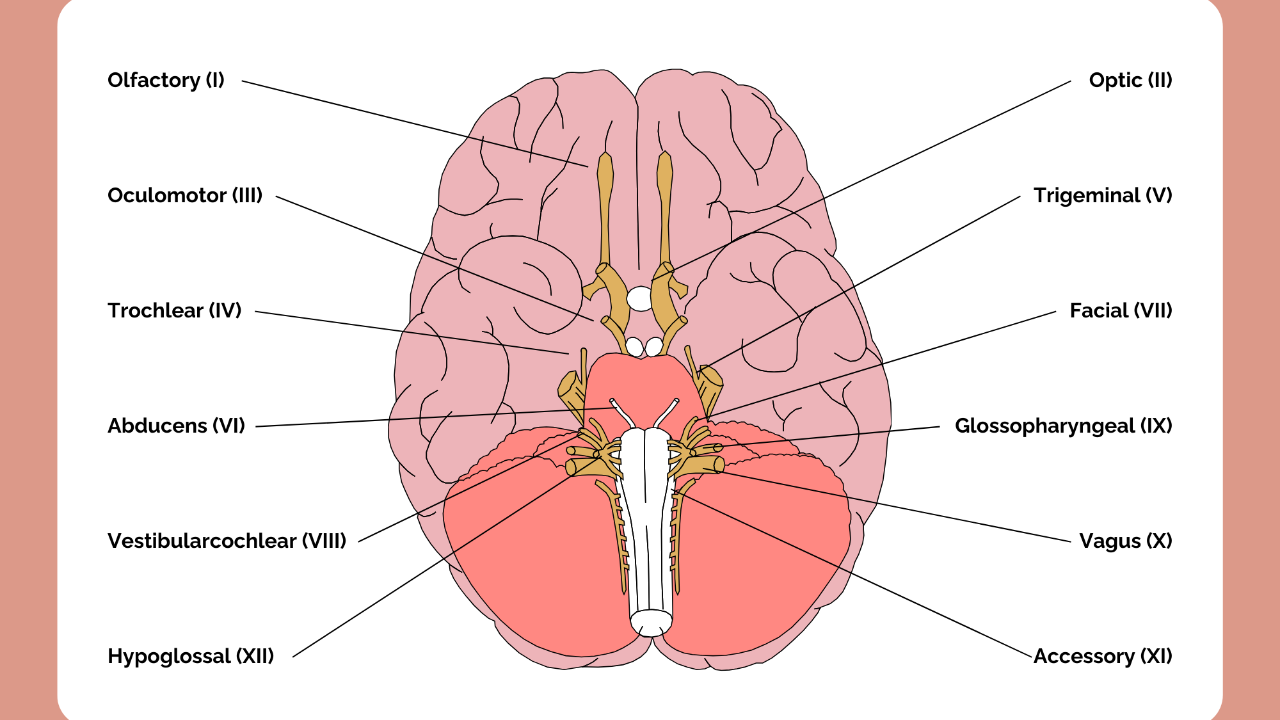
A Summary for Yoga Teachers
For the last decade, Polyvagal Theory has been the language of trauma-informed yoga. You may be familiar with some of these terms even if you haven't studied the theory directly: ventral vagal safety, dorsal vagal shutdown, co-regulation, the social engagement system, the ladder of nervous system responses. These concepts have worked their way into yoga teacher training programmes, therapeutic frameworks, and the way millions of yoga teachers explain their work to students, including, at times, me.
I had actually planned to write about the hierarchy or ladder of nervous system responses this week, when I came across a significant body of scientific critique that called this very idea, and much more of Polyvagal Theory, into serious question. Rather than write the post I had planned, it felt more honest to sit with this research and try to summarise what it means for those of us teaching in this space.
The papers
In early 2026, a consensus paper authored by 38 of the world's leading specialists in vagal physiology, autonomic neuroscience, and vertebrate evolution was published in the journal Clinical Neuropsychiatry, titled Why the Polyvagal Theory is Untenable (Grossman et al., 2026). This followed an earlier detailed evaluation of the five core premises of Polyvagal Theory by the same lead author (Grossman, 2023), which reached similarly critical conclusions. Together, these papers represent not a fringe dissent but the considered view of the field's leading experts, built on experimental evidence accumulated over 45 years.
Their conclusion was not that Polyvagal Theory is incomplete or partially correct. It is, in their assessment, untenable, meaning it cannot be defended on the basis of existing neurophysiological and evolutionary evidence.
As yoga teachers, particularly those of us who teach trauma-sensitive or nervous system-oriented approaches, we need to understand what this means. And we need to be willing to update our understanding, even when that means putting our hands up to having taught something that didn't hold up.
What Polyvagal Theory actually claims
Developed by Stephen Porges from the 1990s onwards, Polyvagal Theory proposed a three-level hierarchy of autonomic nervous system responses. The ventral vagal system, associated with a specific brainstem nucleus called the Nucleus Ambiguus, was said to mediate safety, social engagement, and co-regulation. Below it sat the sympathetic fight-or-flight system. At the bottom of the hierarchy, the dorsal vagal system, the Dorsal Motor Nucleus, was presented as a primitive, evolutionarily ancient pathway mediating shutdown, freeze, and dissociation under conditions of extreme threat.
This ladder of responses gave yoga and therapy communities something genuinely seductive: a neurophysiological story that explained why breathwork, felt sense, and somatic practice help people heal. The vagus nerve became the protagonist of trauma recovery, and many of us built our teaching around it.
Where it falls apart
The scientific critique covers five core claims. Here are the four most relevant to yoga teachers.
Claim 1: The ladder of nervous system responses does not exist as described
The dorsal and ventral split that sits at the heart of Polyvagal Theory does not hold up to scrutiny. Decades of experimental evidence, including studies using the most precise neurological tools currently available, techniques that can stimulate individual groups of neurons with extraordinary accuracy, consistently show that the ventral nucleus is responsible for virtually all vagally mediated heart rate control, including during defensive and freeze states. When researchers directly and precisely stimulated the dorsal nucleus, heart rate barely changed. One senior researcher involved in this work noted that an equivalent level of stimulation applied to the ventral nucleus would likely stop the heart entirely.
This means the three-level ladder of nervous system responses that so many yoga teachers have been trained in, ventral vagal safety at the top, sympathetic fight and flight in the middle, and dorsal vagal shutdown at the bottom, is not supported by the evidence. The hierarchy, as described by Polyvagal Theory, does not exist.
The concept of dorsal vagal shutdown, perhaps the most widely taught idea in trauma-informed yoga, has no evidentiary basis in humans. Studies of emotional freezing and dissociation in humans show either no significant change in heart rate or very small decreases. The idea of massive, life-threatening slowing of heart rate caused by dorsal vagal activation, which Polyvagal Theory presents as the physiological basis of shutdown, has never been demonstrated in human research.
Claim 2: Heart rate variability does not measure what we have been told it does
The measure known as HRV in wellness contexts, technically called respiratory sinus arrhythmia or RSA, has been presented by Polyvagal Theory as a direct window into vagal tone and therefore into nervous system state. The researchers describe this as a fundamental category error, one that confuses an indirect and approximate index of one small aspect of cardiac vagal activity with the whole phenomenon of vagal tone.
HRV is influenced by breathing rate and depth, sympathetic nervous system activity, blood pressure, carbon dioxide levels, ageing, body position, and multiple other factors. It cannot reliably tell us what the vagus nerve is doing. This matters practically because HRV monitoring has become deeply embedded in wellness culture as a measure of nervous system health, and Polyvagal Theory is the primary reason so many people believe it works that way.
Claim 3: The evolutionary story is wrong
Polyvagal Theory claims that myelinated vagal fibres, which enable rapid and flexible heart rate responses, are unique to mammals, and that this neurological development gave us our distinctively mammalian capacity for social behaviour. Multiple independent lines of evidence show that fish, sharks, lungfish, amphibians, reptiles, and birds all possess myelinated vagal fibres with rapid conduction velocities. Non-mammalian vertebrates also demonstrate complex social behaviour, including pair bonding, cooperative parenting, social learning, group vigilance, and emotional communication. The characterisation of reptiles as socially primitive and neurologically underpowered, which sits at the heart of Polyvagal Theory's evolutionary claims, is simply not supported by the comparative biology evidence.
Claim 4: The psychological concepts were not originated by Porges
The ideas that give Polyvagal Theory so much of its therapeutic appeal, including psychological safety, co-regulation, trauma freezing, dissociation, and social engagement, all come from prior work in attachment theory, non-directive psychotherapy, and trauma psychology, predating Polyvagal Theory by decades. Porges' contribution was to attach these existing and valuable concepts to a physiological mechanism. That mechanism is what doesn't hold up. The concepts themselves, and the practices built around them, have a legitimate independent history.
On the question of critics and complexity
It is worth addressing directly how Porges has responded to scientific criticism over the years, because it tells us something important. When challenged by physiologists and neuroanatomists, his primary response has been to suggest that critics have not properly understood his theory. He has tended to reference his own publications in response to criticism rather than engaging with the experimental evidence being raised. The 2026 paper also documents a significant number of citation errors, papers attributed to the wrong authors, published in the wrong journals, and in several cases papers cited as supporting Polyvagal Theory that, when read carefully, actually contradict it.
One has to ask: if a theory is so subtle and complex that decades of leading experts across multiple disciplines have consistently misunderstood it, is it actually a useful clinical or educational framework? A theory that cannot communicate clearly enough to be accurately evaluated is not a strong foundation for teaching vulnerable people about their own nervous systems.
What Polyvagal Theory leaves out: the rest of the brain
One of the most significant limitations of the theory is its narrow focus on a single nerve when emotional regulation, trauma, and healing involve a distributed, whole-brain-body system.
The amygdala, the brain's primary threat-detection centre, triggers fear responses faster than any vagal mechanism and communicates in both directions with the prefrontal cortex, which handles context, decision-making, and regulation. Trauma profoundly affects this relationship. Chronic threat can suppress prefrontal regulation, which is what allows us to contextualise our experience and respond rather than simply react. The HPA axis, which governs cortisol and the broader stress hormone cascade, is arguably more central to trauma physiology than anything vagal.
Interoception, which is the brain's perception of internal body signals, is processed through the insular cortex and anterior cingulate cortex and is directly and powerfully relevant to somatic yoga practice. Research in this area offers one of the most evidence-based explanations available for why body-based practices help trauma survivors: yoga appears to build insular sensitivity and support prefrontal-amygdala regulation. None of this requires Polyvagal Theory.
What is a regulated nervous system, really?
This is where we need to be most careful in our teaching, because Polyvagal Theory may have given us a subtly misleading picture of what we are actually working toward.
A healthy nervous system is not a calm one. It is a flexible, adaptable one. The entire point of the autonomic nervous system is its responsiveness. It is designed to mobilise under threat and return to baseline when the threat has passed. The goal of yoga practice and trauma-informed work is not to keep people in a ventral vagal state. It is to expand their capacity to move across the full range of nervous system states and return without getting stuck.
The Window of Tolerance model, developed by Daniel Siegel drawing on Pat Ogden's somatic work, captures this far more accurately. It describes a zone of arousal within which we function with full cognitive and emotional capacity, and recognises that trauma shrinks this window while recovery involves expanding it and improving the arc of return between states. This model maps cleanly onto what we actually know about prefrontal-amygdala regulation, arousal physiology, and autonomic flexibility. It does not require any inaccurate neurophysiology to hold together.
What this means for our teaching
The therapeutic practices we use are not discredited by this critique. The researchers explicitly acknowledge that somatic and trauma-informed practices may genuinely benefit people. Felt safety, body awareness, breathwork, co-regulation, and autonomic attunement are real, valid, and important. What we do not yet fully understand is the precise physiological mechanism behind why they work.
What we do need to stop is presenting Polyvagal Theory as established neuroscience, particularly in teacher training. When we train other teachers, people who will go on to teach vulnerable populations, we have a responsibility to distinguish clearly between what we observe experientially and what is supported by robust evidence.
Rather than telling a student they are in a dorsal vagal state, we might simply say their nervous system has moved into a protective shutdown response. The experience they are having is real. We describe it honestly, without attaching a physiological explanation that the scientific community has now rejected.
Our practices can stand on their own. They do not need a framework that has been comprehensively dismantled. More honestly, they deserve a better one, and that science does exist, in interoception research, in prefrontal-amygdala regulation studies, and in the neuroscience of breathwork and movement. It is less elegantly packaged than Polyvagal Theory. It is also true.
Want to go deeper?
I will be updating how I present nervous system science in my teacher training programmes. For those of you with access to the Yoga for Anxiety and Trauma online course, a new video exploring this will be coming soon. For those interested in joining the 300-hour Advanced Teacher Training, we will have the time and space to work through this research and what it means for evidence-based trauma-sensitive teaching in much greater depth.
References
Grossman, P., Ackland, G.L., Allen, A.M., Berntson, G.G., et al. (2026). Why the polyvagal theory is untenable: An international expert evaluation of the polyvagal theory and commentary upon Porges, S.W. (2025). Clinical Neuropsychiatry, 23(1), 100-112. https://doi.org/10.36131/cnfioritieditore20260110
Grossman, P. (2023). A critique of polyvagal theory: An evaluation of polyvagal theory's basic premises and a review of evidence regarding its central assumptions about RSA, vagal function and vertebrate evolution. Biological Psychology. https://doi.org/10.1016/j.biopsycho.2023.108511
Grossman, P. and Taylor, E.W. (2007). Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biological Psychology, 74(2), 263-285.
Siegel, D.J. (1999). The Developing Mind. Guilford Press.
Taylor, E.W., Jordan, D., and Coote, J.H. (2022). Central control of the cardiovascular and respiratory systems and their interactions in vertebrates. Physiological Reviews.
Like what you've read?
Sign up to my newsletters and I'll share new articles with you. Plus you'll be the first to hear about my upcoming classes, courses, workshops and offers, and you'll receive my free bandhas video in your welcome email.
I respect your privacy. I won’t bombard you, and I won’t share your details. View my privacy policy for more information.
